
The facts and figures for lateral ankle sprains:
Most common acute sports medicine injury
– 53% of all basketball injuries Garrick et al (1983)
– 21% of all soccer injuries Ekstrand & Tropp (1990)
– Estimated to be >23,000 ankle sprains/day in the USA
– The lateral ankle ligaments are not as thick as the medial ankle ligaments therefore there is increased incidence of lateral ankle sprains.
The video below highlights the anatomy of the ankle complex
The mechanism of injury
~85% of all ankle sprains involve a supination injury mechanism (Funk, 2011)
– Combinations of ankle/foot plantar flexion, inversion and adduction.
– It is less common for these injuries involve to involve an external force.

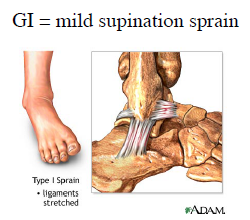
What grade is your ankle sprain?
Grade 1 –
1. Partial tear of the ligaments
2. Mild bone bruising
3. Ability to weight bear through the ankle
4. Return to sport approx 11 days
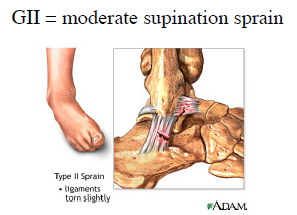
Grade 2
1. Complete tear of the Anterior talofibular ligmanet and partial tear of the calcaneal fibular ligament
2. Moderate bone bruising
3. Able to weight bear but with disrupted gait pattern
4. Return to sport 2-6 weeks
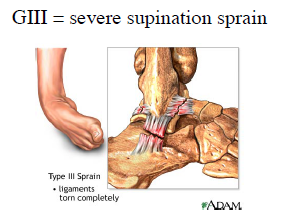
Grade 3
1. Complete tear of the Anterior talofibular ligament and calcaneal fibular ligament +/- Posterior talofibular ligament
2. Common and severe bone bruising
3. Intolerant to full weight bearing
4. Return to sport 4 – 26 weeks
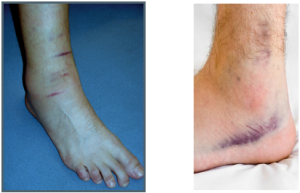
Signs & Symptoms of a lateral ankle sprain:
Initial Management of the Acute Ankle Sprain

1. On arrival at Physio Tullamore a thorough history will be taken to determine the mechanism of injury. A hands on assessment will be performed using the latest evidence based assessment techniques. If there is a suspected fracture a referral for the emergency department will be given.
2. If there is no fear of a fracture the main aim is to reduce the Pain & Swelling – Anti-inflammatory medication can help reduce inflammation caused by the damaged tissue. Along with this we use an Ice Compression system at Physio Tullamore to reduce the swelling.

.jpg)